


Claire raised her arms above her head and did a cartwheel on the balance beam. Her ten-year-old body was taut and strong, her limbs flowed like water from pose to pose in her gymnastics routine. Watching this magnificent girl, you wouldn’t suspect that she had recently used those powerful legs to kick her mom across the room because she’d told Claire to get up and go to school.
Getting to school has been a problem for Claire; she was late 54 times last year. And just the night before, she had broken the bow of her violin in a tantrum sparked by a careless remark by her dad. In fact, she’s destroyed many things, like a portable DVD player she couldn’t get to work. She’s taken scissors to her hair and clothing — and once brandished them during a play date.
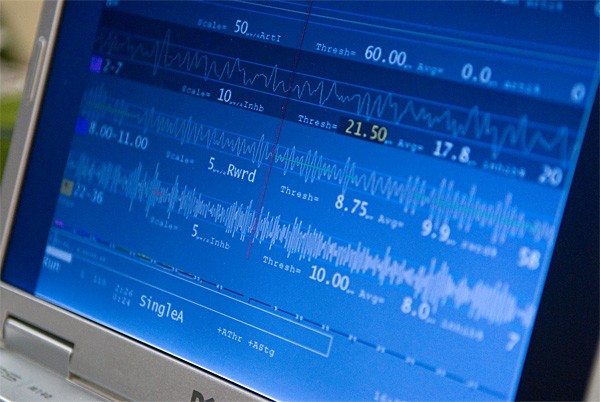
By studying brain waves, doctors have been able to measure the differences in the brains of children exposed to early trauma. Credits: Chris Duffey 
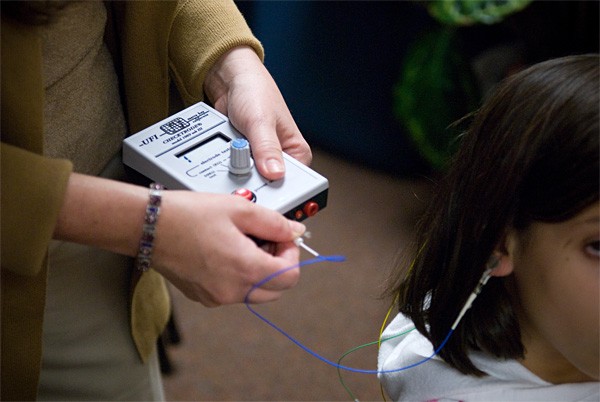
Nurse and neurofeedback practitioner Lori DiRicco. Credits: Chris Duffey A neurofeedback session. Credits: Chris Duffey Elena during one of her visits to Lori DiRicco. Credits: Chris Duffey


Claire is a challenging child. But that shouldn’t be too surprising. She was abandoned in a market in South China when she was three weeks old, and spent the next twelve months in the municipal orphanage. “They showed us the room she lived in, maybe ten or twelve babies in little cribs,” recalled Barbara, her adoptive mother. “There were rows of small cribs with rails maybe a foot high. They didn’t let them crawl or walk, so they didn’t need to have high rails. When they put them in high chairs, they’d just sit there.”
After struggling for years to get pregnant and spending $16,000 on in-vitro fertilization, Barbara and Steven Pirelli had traveled from Oakland to China to adopt. They were drawn by nothing more than a single color snapshot. The baby they met was dirty and painfully thin: just fifteen pounds. From the waist down, she was atrophied. She couldn’t crawl, roll over, or sit up, and didn’t make eye contact. But Barbara and Steven didn’t care. “You’ve waited so long, you’re not going to say no,” Barbara said.
While the couple had been warned about what physical condition to expect, they hadn’t been prepared for Claire’s strangely detached personality. She was friendly to everyone — inappropriately so when she got older — but not especially bonded to her new parents. When she started preschool, all the other toddlers cried and clung to their parents when they were dropped off, but Claire happily ran off to the swings without a backward look.
But as she got older, she developed a mean streak. She’d make one girl in her group her best friend and reject the rest. In 2005, on a fourth-grade class trip, away from adult supervision, she pushed another girl down and kicked her. Notes from teachers got more pointed; the word “vicious” was used.
When Claire was only two, a psychologist friend of Barbara’s who also had adopted a baby from China had warned her that Claire needed help. Now, years later, it finally sank in.
“Oh My God, I Found It”
On a recent sunny afternoon, Elena emerged from the gaggle of fourth graders at her school on a hilltop in Pleasanton. She has soft brown hair, fair skin, and a lanky frame that’s helped her become a starter on her school’s soccer and basketball teams. She couldn’t wait to tell her mom everything: how she did on her math test, what she wrote, what her friends said and did. Walking back to the SUV for the short trip home, she said, “Mom, I’m getting my hopes up about Chrissie coming on Friday. I’m getting my hopes up — but I’m trying not to keep my hopes up too much, so if Chrissie doesn’t come over, I won’t be too disappointed.”
“It sounds like you’re doing good in school and being fun to be around, so it just might happen,” said Betty, her mom.
While some nine-year-olds live in a whirl of sleepovers and play dates, having a friend come over is a hard-won privilege for Elena. The four years she spent bouncing from a Romanian orphanage to a series of foster homes took their toll, cognitively, emotionally, and physically.
“She was so tiny, only 28 pounds,” Betty recalled. “She didn’t have much hair. She had ringworm, and couldn’t speak.” Betty thinks Elena was kept swaddled for the first year of her life; when they met her in the foster home, she was three years and nine months old and still sleeping in a bassinet.
Betty and Howard Sundahl had an American-dream life: Their biological sons, now ages eighteen and sixteen, were growing up strong and healthy. Their house, in a development of million-dollar homes, had all the right stuff, from the granite in the kitchen, to the swimming pool and terrace out back, to the two dogs lounging on their special cushions in the comfortable family room. “We wanted to give thanks for everything we have here and we wanted to do something to make a difference,” Betty said. “I wanted a little bigger family, and I thought taking care of a little girl that’s already on the earth would be better than bringing a new one. We chose Romania because the children there were in more need.”
In her first year with her new family, Elena had some speech problems; they chalked that up to her getting used to a new language. But by her second year, it was clear that something wasn’t right. Elena’s silence gave way to incessant chatter. In kindergarten, she had trouble staying in her seat, seemed to have no sense of personal space, and constantly interrupted in class. “We wanted her to bloom here, and it just didn’t really happen until we got into some therapy,” Betty said
Betty took her to specialist after specialist, and each gave her a different diagnosis and treatment recommendation — autism, sensory integration disorder, auditory processing difficulties, attention deficit hyperactive disorder. Finally, a pediatrician suggested in passing that she might want to see an attachment therapist.
“I came home and Googled attachment therapy, and up comes this list of symptoms,” Betty recalls. “I said, ‘Oh my god, I found it. This is it.”
“Why Did This Happen to Me?”
Both Claire and Elena were diagnosed with reactive attachment disorder, a controversial psychiatric label that was added in 2002 to the Diagnostic and Statistical Manual of Mental Disorders, the psychiatrist’s bible. In their first post-adoption years, they showed many of the symptoms of the disorder: unwillingness to make eye contact, difficulty connecting with others, painfully anxious or ambivalent about receiving attention and love. Such kids are like seeds planted in concrete. They’re unable to absorb the love they’re offered — and they’re furious about it, too.
Clearly, not every adopted child experiences attachment problems. “The vast majority of adopted kids are doing fine,” said David Brodzinsky, an Oakland clinical psychologist and Donaldson Institute project director.
But Nancy Curtis, medical director of the International Adoption Clinic at Children’s Hospital, said all the kids she sees have developmental delays. “We know they will be delayed because of environmental reasons,” she said. “They’ve been raised in institutions.” The parents who come to Curtis are self-selected; most have at least an inkling that something is wrong. Neither does her clinic have stats on what percentage of the children do catch up without special treatment. But in general, she said, the kids she sees have gotten sicker over the past ten years, as the sending countries have moved down the economic scale.
According to Families with Children from China, as many as 25,000 people are on the waiting list to take infants, toddlers, and children as old as ten from Chinese orphanages. In fact, foreign adoptions are cleaning out institutions in China, South Korea, and Eastern Europe; the number of waiting parents may exceed the number of available children.
Some of these adoptive parents find themselves with little monsters on their hands. Their kids don’t show affection, and they reject hugs and kisses. The simplest request, like, “Put on your shoes so we can go to the store,” is met with defiance. Attempts to set limits provoke tantrums that last for hours. A child may sneak things, deliberately break things, even steal things. Sometimes the anger gives way to incessant demands for attention, but no amount of attention can calm them. They sometimes hoard food; they might try to hurt siblings; they may even creep into their parents’ bedroom in the night armed with a knife.
Their parents wonder, with grief and rage, “Why did this happen to me?”
These children aren’t evil. They’re reacting appropriately, in the best way they can, to the trauma and neglect they’ve experienced in their early lives. They may have been beaten or abused in the institution; they may have been neglected, which is just as harmful. In baby warehouses, they lie in cribs 24 hours a day, being fed and changed on a rigid schedule by people who see their work as a factory job. They cry and cry, but no one comes.
The depth of this problem has been revealed in the past decade, as neuroscientists have begun to chart the abnormalities in these kids’ brains. Functional magnetic resonance imaging studies let researchers see which parts of the brain become active when someone does mental tasks such as arithmetic or looking at a video of his mother.
Victor Carrion, director of the Stanford Early Life Stress Research Program, has done several brain imaging studies that show how stress, trauma, and abuse alter the brain. He has found significant differences in the brains of children who had experienced trauma, compared with those of unharmed kids. The hippocampus, important for learning, memory, and emotion, was smaller; other parts of the brain seemed to be larger than normal.
When Michael De Bellis, a Duke University psychiatrist, studied the brains of fourteen children diagnosed with post-traumatic stress disorder, he found their brains were smaller than the normal control groups, and the corpus callosum, the band of nerve tissue that lets the two hemispheres communicate, was also smaller. The children with PTSD had trouble solving problems and using abstract reasoning, and they showed definite deficits in putting concepts into words. While their psychomotor speed was as good as the control group’s, their visual and spatial skills were weaker.
It’s hard to get a handle on how many children adopted from abroad suffer brain damage that will lead to emotional disorders. Adoption organizations don’t want to put off prospective parents or damage sometimes-tenuous relationships with overseas orphanages. Adoptive parents whose kids start to struggle don’t necessarily report back to the adoption agency.
When the Evan B. Donaldson Adoption Institute, a not-for-profit organization devoted to improving adoption policy and practice, did a study of children adopted from foster care in the United States, it couldn’t get accurate numbers from state agencies, and the kinds of data states did report wasn’t consistent.
Parents may assume — as they’re told over and over — that all they need to do is love and be patient. But lots of love and the most devoted parenting won’t help certain kids. They’re simply unable to respond, because their brains never developed the connections and responses that allow them to feel empathy, trust, and connection. Instead, their nervous systems are locked into a state of dread, ready to panic at a hint of stress.
However, their situation is far from hopeless. The same brain-scanning technology that found damage also has shown that the brain can continue to grow and change throughout our lives. While they may be impervious to love and psychotherapy, kids like Claire and Elena can benefit from a variety of treatments — some confirmed by science, others still considered woo-woo — specifically designed to rebuild their brains.
Shaping the Brain
At birth, human babies are the most undeveloped of mammals. A full 30 percent of the brain’s growth takes place after birth, especially in the first three years of life. This development can be thwarted or twisted by trauma or neglect.
Think of the infant brain as a tomato seedling. The little three-leaved plant has the potential to grow into a lush shrub covered with juicy fruit. But you can see its history in the shape of the full-grown organism. If sun only hit it on one side, that side is bright green and strong, while the side in the shade has only a few yellow leaves. If it didn’t get much water, the tomato plant is small and tough; if it was alternately drowned and parched, it’s stunted.
This is how a baby’s brain develops in response to experience — and specifically, in response to care from his mother. This first relationship forges the neural pathways that shape the responses of the brain system that handles all the complexity of human interaction. In this context, mother should be seen as a role and not a biological state, and mothering is the sum of all the nurturing and care an infant receives. Anyone can provide mothering: a single dad, an adoptive parent, an older sibling, a nanny — or an orphanage worker. The key for a baby is having one person he can count on to be there for all his needs, physical, cognitive, and emotional.
Oxytocin, the hormone that stimulates the contractions of labor, is key to the bonding process between mother and baby, as well.
“Every time a mother picks up the baby and spends time breast-feeding or bottle feeding, she produces oxytocin, and it brings on an increasing amount of affection to the baby,” said Marshall Klaus, an adjunct professor of pediatrics at UCSF. “And suddenly she loves the baby much, much more.”
Klaus and his wife, Phyllis Klaus, a psychotherapist, are two of the foremost authorities on how babies learn to love. The Berkeley residents co-authored, with John Kennell, Bonding: Building the Foundation of Secure Attachment and Independence (Perseus 1995).
“Oxytocin raises the pain threshold, and it creates a sense of calm, reducing the stress hormones in mother and baby,” said Phyllis Klaus. The baby learns — at the physiological level — that the world is a comforting, safe place. At the same time, connection with Mommy paves the way for the proper development of cognitive abilities, and it will set his emotional thermostat to a nice, even temperature, so a child will be neither hotheaded nor fearful. Oxytocin will foster the healthy development of the prefrontal cortex, the seat of judgment and rationality, giving a child the ability to think before he acts and to curb his impulses when necessary.
On the other hand, if the baby doesn’t experience mothering — if, instead, he experiences fear, abandonment, and deprivation — his brain development will be too influenced by cortisol, the fight-or-flight hormone.
“Chronic stress during childhood leads to heightened responsivity to stress and an increased risk for adult mental health problems,” said Allan Schore, a clinical psychologist on the faculty of the Department of Psychiatry and Biobehavioral Sciences at UCLA and authority on postnatal brain development.
There are adaptive advantages to a brain completing its development in response to postnatal experience. As humans spread out from the plains of Africa, encountering different environments and experimenting with new ways of living, babies born to nomadic desert tribes were able to develop in ways that suited their people and the land, while the children of farmers could develop brains that fit their people’s ways.
But the brain of a baby born into deprivation and neglect will adapt to that milieu, leaving him at a loss to cope with the suddenly overwhelming environment of a new family in one of the most stimulating regions on the planet.
An Elusive Diagnosis
Because most parents don’t get to watch their children’s brains on a scanner, very early signs of maldevelopment, such as a baby not responding to smiles or play, may be seen as simple delay. It’s when they start school that many parents realize there’s a bigger problem. Attention deficit hyperactive disorder, or ADHD, is often the first diagnosis for troubled adoptees. If medication doesn’t do enough, parents can get on a therapy treadmill, going from therapist to nutritionist to psychiatrist to therapist. It usually takes a while until they enter the world of attachment therapy.
While adopted children may have symptoms of ADHD, it’s often not the right diagnosis, believes Virginia Keeler-Wolf, a therapist and founder of the Family Attachment & Adoption Center East Bay. Their nervous systems have been set to high alert by the distress of not having a mother to cling to. “They show a lot of hyper-vigilance,” she said. “They’re noticing footsteps above them, things going on outside the window, instead of paying attention in class.”
This hyper vigilance was a survival skill. A baby abandoned on the street and then left alone for hours at a time had a better chance if she could catch the attention of a caregiver as he made his rounds — or evade the attention of the more brutal ones. As they grow up, even though they’re now safe with their adoptive families, these children overreact to the tiny stressors of daily life. The tantrums, control-freaking, and lashing out so many adoptees go through are the result of the cortisol and adrenaline shooting through their nervous systems.
The flip side of this syndrome is often overlooked. Their brains never got a chance to release oxytocin in response to mothering. Now, they can’t open up and trust their parents, so they can’t be soothed.
Traditional talk therapy — and even the child-friendly play therapy — doesn’t work for people with attachment disorders, says Susan Love, a psychotherapist who heads the Bay Area Attachment Center in Oakland. “A child is not available to enter into a relationship with a therapist if they have not developed one with the parents.”
Attachment therapy is a term that encompasses a variety of strategies designed to build the ability to bond. “By the time families get to me, they’re pretty worn out,” Love said. “They feel like they’ve failed as parents, and they’re angry. They’re ready to work because the first thing we can offer them is hope that you can have a different kind of life with your child.”
This is work that involves not only the child, but also everyone in the family. Mom and Dad need to learn to do what’s known as “therapeutic parenting,” relating to their child in ways that help heal the wounds, attachment therapists say. It may mean taking a hard look at some of their own issues. Mainstays of parenting like time-outs and consequences don’t work on kids with reactive attachment disorder. Children with attachment disorder need their parents to set firm boundaries and prove that they can or will take care of them, yet they’re constantly testing those boundaries and trying to make their parents fail. If the parents respond by getting angry, shutting down, or feeling guilty, they can’t effectively show their children how to regulate their own emotions.
Regulation doesn’t mean regimentation or rigid rules. “It means helping them calm down,” said Phyllis Klaus, who specializes in helping children learn to attach to their parents. “It’s an internal shift from being stressed out and chaotic.”
The Sundahls took Elena to see Virginia Keeler-Wolf, a therapist who specializes in helping kids traumatized by adoption or foster care. She helped them understand why love was not enough for Elena.
Keeler-Wolf’s techniques included holding therapy, a controversial technique in which Betty held Elena in her arms like a baby and tried to keep eye contact with her as the six year old struggled to get away. Sometimes she and Howard fed Elena with a bottle or popped chocolate in her mouth. The theory is that a child who missed these mothering experiences needs to go through them in order to learn to bond.
At first, Elena hated it. Like many formerly neglected kids, she feared the loss of control and feelings of vulnerability evoked by being held. Eventually, she began to enjoy it; now, she looks forward to it and lets Betty know when she wants some holding time.
Retraining the Brain
In 2004, when she was in second grade, Claire’s teacher insisted to Barbara that she get help. Claire was hyper and disruptive in class. She began taking Concerta, an extended-release form of Ritalin, for ADHD. “It was night and day, an incredible difference,” Barbara said. Not only did it help her focus and stay calm, but she got along better with other children. That fall, they added occupational therapy for sensory integration, which involved things like brushing Claire’s skin with different textured materials, such as a loofah or yarn.
By spring 2005, Claire’s normally upbeat disposition had changed. Her gymnastics coach and teachers at school independently told Barbara and Steve that she seemed depressed. They started attachment therapy, but the therapist wasn’t a good fit for any of them. In September 2006, they quit, and Claire began group therapy for adopted girls with Virginia Keeler-Wolf.
At the same time, Barbara and Steve also began therapy with Keeler-Wolf. Their sessions were a mix of reflection on their own feelings and practical advice about how to deal with Claire in ways that would make her feel more secure and not provoke her anxiety. For example, the therapist explained that it’s important not to shame Claire or make her feel she’s bad when she acts up. She suggested that when Claire did something inappropriate, instead of asking her to apologize — which didn’t mean much to her — Barbara should have her perform a chore to help her out. Sweeping the porch or folding laundry helped teach Claire reciprocity.
“Until we figured out that Claire had both ADHD and attachment issues, I really thought I was a bad parent,” Barbara said. “I have a lot to learn, and I am certainly not perfect, but I now have a better understanding of Claire, and I don’t blame myself as much.”
Early this year, Claire embarked on still another course of treatment with Lori DiRicco, a nurse and neurofeedback practitioner. Neurofeedback is a more refined form of biofeedback that trains the brain to produce patterns that are closer to normal. In a neurofeedback session, which could last from 20 to 45 minutes, DiRicco attaches sensors to the child’s head and ears. These sensors connect to an electroencephalogram device that translates the signals into a graph for the therapist and a computer game for the child.
For children with ADHD, hypervigilance, or an inability to control their impulses, the goal is to strengthen the cortico-thalamic loop, a neural circuit that connects the neocortex, the “thinking brain,” to the parts of the brain that regulate emotion. In healthy functioning, the rational brain sizes up an everyday situation and signals the emotional center that all is well. When a child is born into fear or chaos, connections in that loop may be weak or nonexistent, so every situation is read as scary.
DiRicco explains that her treatment goal is usually to help “wake up” the frontal lobe, the part of the brain that plays the major role in inhibiting behavior. “When their frontal lobes are working better, they’re able to stop this impulsive behavior,” she said.
The child actually plays the game with his brainwaves. For example, in a Pac-Man-like game, when the brain enters the desirable state, colored dots disappear from the screen. Consciously trying to make the dots disappear doesn’t do any good; in fact, it may impede reaching the goal because the thinking brain is getting in the way. You could think of neurofeedback as a gym for the brain. Said DiRicco, “The more you practice something, the neural pathways in the brain get bigger and more efficient.”
Elena also receives neurofeedback training from DiRicco, and she recently began neurodevelopmental training with Emily Beard Johnson, a practitioner who travels to the Bay Area from her home base at the Northwest Neurodevelopmental Training Center in Salem, Oregon. This therapy was originally developed to rehabilitate stroke victims, using simple, repetitive movements to rebuild pathways damaged by the clot. But it also shows promise for children like Elena, who weren’t allowed to go through the normal progression from rolling over to sitting up to crawling.
This normal progression of physical abilities also triggers stages of cognitive and emotional development, according to Johnson. Any gap in the developmental sequence will result in impaired neurology and behavioral, emotional, academic, or motor problems. For example, even though Elena now walks, runs, and plays basketball, not going through the crawling stage at the right time could have created deficits in brain function.
After an individual assessment, she was assigned to crawl across the room while keeping her stomach in contact with the floor, as well as some eye exercises that mimic a baby’s initial sight patterns. In all, she does three different sets of sixty movements each, three times a day. Betty gets Elena up 45 minutes early and reads to her while she crawls, popping a jelly bean into her mouth every time she completes a segment.
“If a house has a faulty foundation, you can spend all your time making the doors hang straight or fixing cracks, or get down to the root of it and fix the foundation — and that’s what we do,” Johnson said.
Some medical professionals are leery of these alternative therapies. Said Nancy Curtis, an MD and head of the Children’s Hospital International Adoption Center, “Emerging therapies can sometimes be very promising, but, as a parent and doctor, I’d say you want the therapy being used to have some basis in science. There are a lot of therapies that someone thinks is a good idea [which] may actually be not useful.”
The concept of attachment therapy itself has come under fire following the deaths of several children whose parents said they were following the advice of therapists. Usually attachment therapy involves gentle activities such as holding the child in the parent’s lap and feeding him. But there’s no official protocol. Some therapists advocate forcibly restraining the child in the lap, or even lying on top of him and insisting he look into the parent’s eyes. One ten-year-old girl died after she was covered with blankets and held down for an hour in an exercise designed to recreate the experience of birth.
The American Psychiatric Organization recognized reactive attachment disorder in 2002, but it also cautioned that there was no scientific evidence to support the effectiveness of coercive holding therapies, or re-birthing techniques. While having a standard diagnosis helps get insurance coverage, some psychologists think the classification is too broad and fuzzy; others think it stigmatizes kids. DeBellis thinks that post-traumatic stress disorder is a more accurate diagnosis for many of the children who are unable to trust and love, to sit still and pay attention, to learn and play.
“Definitely Worth It”
Betty Sundahl credits the neurological redevelopment work for Elena’s newfound speed as a runner. But it’s the sum of all the therapies that has put Elena on the upswing, she thinks.
“It’s such a long process, that if you have huge expectations for any of these treatments, you will no doubt be disappointed,” she said. While medication remains her mainstay, “I don’t know what is really working the best. I’m throwing a lot of things at it, and she’s changing and learning and growing all the time.”
Indeed, while they may still struggle with regulating their emotions, in many ways, Claire and Elena are thriving. That’s because the brain continues to grow and develop through early adulthood — and even beyond. “Even though there have been some missed opportunities, the brain is capable of repair,” Phyllis Klaus said.
Elena is keeping up with her fourth-grade classes, enjoying play dates and sleepovers, and blossoming as an athlete. Claire has only been late for school twice this year. More important, she maintains a 4.0 GPA. In addition to being the youngest girl on her advanced gymnastics team, she’s becoming an accomplished musician.
Parents of kids with reactive attachment disorder may have gotten more than they bargained for, but that goes for the good stuff, too. “We are so lucky to have her in our lives,” said Barbara. “It has been incredibly difficult and exhausting, but Claire is definitely worth it.”
Neither does Betty have regrets about adopting Elena — although she does regret that they weren’t given more information and support at the beginning.
If they hadn’t adopted Elena, she said, “I would always wonder where that little girl was that I was going to try to save. I just wish I could do it over again, knowing what I know now. I think I could help her so much faster.”
The names of the families, and certain identifying details in this story, have been changed to protect the children’s privacy.







